Conversation with Your PCP
by Diana C.
The conversation with your PCP document to follow is a draft letter which I wrote to help DSers communicate with their PCPs and other doctors about their surgery and about the need for communication between them and their medical care providers. Please feel free to revise, personalize, tone down, or otherwise adjust for your needs. You may want to update the list of annual labs; for example, adding copper, vitamins K and E.
[shaking hands] Hello Dr. _________. My name is [use FULL name]. Before we start our relationship, I think it is important that you understand a fundamental fact about me and my medical history. I have had a form of bariatric surgery known as the duodenal switch. I spent <months, years=””>studying this procedure as well as other bariatric surgeries before I decided the duodenal switch was the right surgery for me. I feel quite confident that I am knowledgeable about my surgery and my post-op care. I hope that you will agree to become educated about it if you undertake my care. It is of CRITICAL importance to me that you do not dismiss my knowledge or concerns, and that you treat me with respect regarding these matters, so if this is not something you are comfortable with, please let me know now so that I can find a doctor who can “work with me.”
Please understand up front the duodenal switch is not the RNY gastric bypass surgery. It is a very different surgery and my needs and life style post op are very different from someone who has had the RNY.
The duodenal switch procedure is actually a two part surgery, including a vertical sleeve gastrectomy and the duodenal switch intestinal reconstruction. Here is a picture of my gastric and bowel reconstruction:
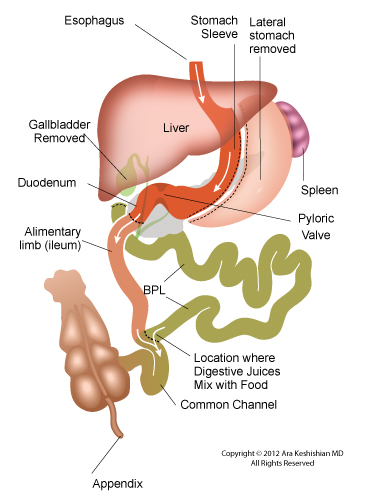
Please note that I have a fully functional, although smaller stomach, so I can still be examined endoscopically just like normal person, at least to the level of the duodenal anastomosis (which may be a side-to-end rather than end-to-end anastomosis as pictured). I can also have a colonoscopy like a normal person, but if I have to have an upper GI, a CAT scan or other procedure that involves visualizing or cleaning out my gastrointestinal tract, I need consideration taken of using smaller volumes of swallowed contrast material or bowel cleansing medium. [depending on your surgery, you might note that you did or didn’t have your gall bladder and appendix removed]
There are some very specific medical issues that I need your help in managing over time, and for that, I need you to understand some of the ramifications of the DS procedure:
- I have had a combined restrictive-malabsorptive procedure in which the restrictive part will substantially resolve over time, but malabsorptive part is permanent.
- Because of this malabsorption, I need regular bloodwork to confirm I am absorbing enough protein, vitamins, and minerals. Please see the list that I have attached of blood tests that I need annually or more often if I am having a problem.
- I malabsorb DIFFERENT vitamins and micronutrients from gastric bypass patients, and I need you to NOT make assumptions based on what you may have read about regarding different procedures. In addition, time-release medications may not be appropriate for me.
- I take a number of supplements [and medications], which I have listed on the attached sheet.
- Fat-soluble vitamin and calcium malabsorption are primary concerns because of the duodenal bypass, and must be monitored closely — and SPECIFIC tests that my surgeon recommends must be ordered routinely — this is NOT negotiable. Calcium must be monitored via PTH and vitamin D3 — perhaps not the usual tests you routinely order for non-DS patients, but none the less I will need this testing frequently and I will need your support in this matter. I may also ask you to provide me with or fax copies of my lab results to my DS surgeon, who has additional expertise in helping me manage my post-op long-term care. A copy of my annual lab requirement is attached.
- From time to time there may be specialized tests that my DS surgeon will request and I will need you to support and respect these requests.
- Other tests, such as albumin, liver function, etc., are also extremely important, as is a baseline and at least every other year I will need a DEXA scan.
- I do not absorb 80% of the fat that I consume, so please do not get concerned that I am eating too much fat. I also malabsorb about 30-50% of the protein and complex carbohydrates I eat, so I must eat more protein than you might think appropriate.
- My primary challenges with living with the DS are, in no particular order:
- Eating 80-100 g of protein/day
- Taking my supplements
- Monitoring my labs to head off any problems as quickly as possible
- Dealing with the stool and gas issues, both volume and smell, which in most cases may be a direct result of my diet: complex carbohydrates, especially white flour, increase the smell and volume of both, and too much fat can cause diarrhea
- Sometimes, constipation is also an issue.
- The intestinal bypass may result in imbalance in the bacterial flora and I may ask you to prescribe unusual antibiotics from time to time — perhaps even prophylactically if I have difficulties with gas and diarrhea – I need to know if you have a problem with this. You may be interested in information I have access to about non-prescription probiotic replacement products that I would be happy to share with you, and which you might find useful with your “normal” patients with intestinal issues such as IBS as well.
- Because I have a normally functioning stomach, I should not have any particular problems with taking NSAIDs or anticoagulants, in contrast with RNY patients.
- NOT every problem I have will be DS-related, just as NOT every problem I had pre-op was obesity-related (an unpleasant and dangerous issue many morbidly obese patients have experienced). Nevertheless, my DS needs to be taken into consideration if problems arise, either as a source of the problem or as a consideration in how medication will be absorbed.
- As with any abdominal surgery patient, I have an increased risk of bowel obstructions, even years after my DS surgery. These can be because of bowel slipping into internal hernias, or holes in the mesentery, as well as into spaces that develop because I have lost abdominal fat. However, there is one very important issue that is particular to the differential diagnosis of bowel obstruction in DS patients (as well as, to a lesser extent, in RNY patients): we can have a complete intestinal obstruction and still be passing stool and gas, because the obstruction can be in the biliopancreatic limb (and thus the alimentary limb could still be fully patent). Thus, it may be necessary to order a CAT scan for me if I present with severe belly pain, even if I am still able to pass stool and gas.
I take the following supplements and medications: [modify based on the supplements and medications you take]
- Calcium citrate: ____ mg/day (this dosage includes ____ mg of Vitamin D, ____ mg of magnesium and ____ mg of zinc)
- Multivitamins: Prenatal (brand), 1/day
- Protonix, a proton pump inhibitor to help reduce the acid in my stomach
- Levoxyl for my hypothyroid
My DS surgeon is Dr. _________, who can be reached at the following telephone number: __________. If I ever have a problem that you feel requires speaking with him/her, please know that s/he can and should be consulted directly. If you feel a HIPAA release is needed, I will be happy to sign one.
If you are interested, I can provide you with additional scientific publications and websites to read. This should be sufficient to let you know what I need out of our professional relationship, and for you to decide whether you can accommodate my request to be an active participant in my health care.
ANNUAL DUODENAL SWITCH LAB ORDERS
Dx: POST-SURGICAL MALABSORPTION, 579.3a
Please Draw the Following:
- CBC
- COMPREHENSIVE METABOLIC PANEL
- FASTING LIPID PANEL
- FERRITIN
- FOLATE
- IRON
- MMA (Methylmelonic Acid)
- PHOSPHORUS
- PTH, intact with Calcium
- TSH
- VITAMIN A
- VITAMIN B6
- VITAMIN B12
- VITAMIN D, 25 HYDROXY
- ZINC
Note:
VITAMIN A REQUIRES 2 ML FROZEN SERUM
VITAMIN B6 REQUIRES PLASMA – FOIL WRAPPED